As the population ages, there are an increasing number of patients who have undergone vascular bypass procedures such as popliteal to anterior tibial bypasses with saphenous vein grafts. Often, in the aging population, the only patent blood vessel to the foot is the bypass graft. When these patients incur injuries or wounds to the most distal aspect of the lower extremity, planning free flap reconstruction can be quite challenging.
I have found that in those patients, magnetic resonance angiography and magnetic resonance venograms can be helpful to establishing a correct plan for the outflow of the microvascular anastomosis. In those cases when the saphenous vein has been used, the surgeon must rely on the venae comitantes of adjacent vessels to determine successful outflow.
I have encountered, that even when native arteries have been diseased, and new blood flow has been established via bypass grafts, the venae comitantes are still often of sufficient caliber. In that case it is important for the operating surgeon to determine the location of the bypass graft tract in relation to the defect, and then select an appropriate venae comitantes in the vicinity of the bypass graft.
Either a long and sufficient caliber leash on the venae comitantes should be mobilized, in addition a flap with a long venous leash that can easily be dissected free of the artery should be selected. I have found the rectus muscle to be an excellent muscle for these cases; In that, the muscle is long and wide allowing not only for adequate coverage, but also for greater margin of separation of vascular bypass and location of nearest venae comitantes.
When the rectus has been harvested, it is important for the surgical team to spend sufficient time and care with the deep inferior epigastric artery and vein to allow adequate mobilization between both vessels.
When there is a single vessel run-off to the lower extremity, I find it helpful to perform the arterial end-to-side anastomosis first so that the flap can be rotated to-and-fro. The vein can then be usually anastomosed so that it will not be kinked. If one anastomoses the vein first, the end-to-side arterial anastomosis is often more difficult as the vein anastomosis now prevents the to-and-fro motion of the flap.
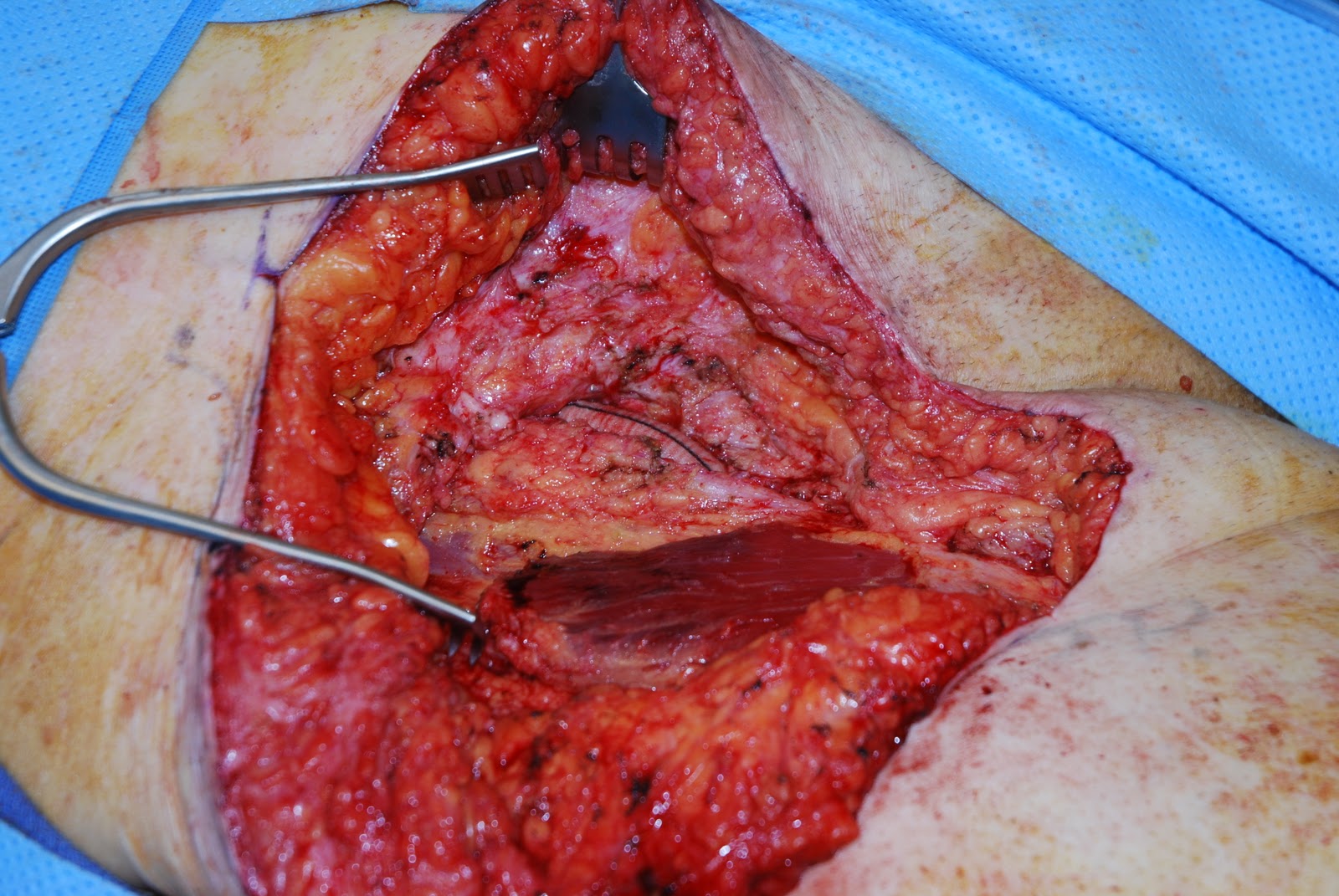
When dissecting toward arterialized vein bypass grafts, I find it helpful to gain proximal and distal control with the vascular bull-dog clamps from the vascular set. One must be aware that there is often a significant amount of scar tissue present around these grafts as they have been tunneled from their proximal to distal locations. Once adequate control has been obtained, the operative surgeons need to spend sufficient time dissecting scar off the vessel before they reach lumen.
Once the muscle has been vascularized, the split thickness skin graft can be placed.